
Artificial Cervical Disc Replacement
The spinal discs in your neck are responsible for helping to shoulder the weight of your head and disperse stress as you bend and twist. Like all moving parts in our bodies, they are prone to degeneration as we age. If a disc is damaged or degenerates to the point that it is shifting out or place or compressing nearby spinal nerves, a surgical operation may be recommended. One of the most common procedures performed for moderate to severe cervical disc degeneration is an artificial disc replacement. A disc replacement does just that – replaces the arthritic disc with a mobile implant. Like hip and knee replacements, they are composed of two small metal plates attached to each side of the joint and separated by a smooth durable plastic spacer.
Who Qualifies for a Cervical Disc Replacement Procedure?
The goal of all spine surgery is to relieve pressure on the nerves and optimize function. Thus, Dr. Jackman starts with the goal to maintain motion of the spine.
The disc replacement procedure is replacing a worn and degenerated disc with a new prosthetic implant. There are patients for whom a disc replacement will not predictably provide a durable, stable, reliable option.
Patients who are not good candidates for disc replacement include:
- Patients with severe facet joint arthritis in addition to disc pathology. A disc replacement will not address the facet joints and they can continue to be a source of pain post-opertively.
- Patients with osteoporosis or osteopenia may not have sufficient bone strength to capably hold the prosthesis is an acceptable position.
If there is instability or a fracture evident, the prothesis may not sit in the perfect position to provide balanced and stable motion. In these and other cases, a fusion may be the preferred alternative.
How Is An Artificial Cervical Disc Replacement Procedure Performed?
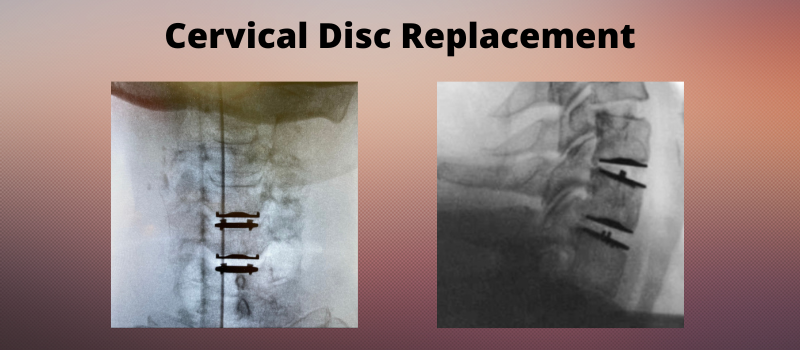
With the aid of a specialized x-ray called a fluoroscope, the surgeon finds the location of the damaged disc and gently retracts the adjacent vertebrae so that the disc can be safely removed. Using a microscope and specialized instruments, the damaged disc is carefully removed. Any offending bone spurs are also removed, and the surgeon may also opt to widen the foraminal opening in the area so that spinal nerves have more room to traverse without being compressed.
The disc space is then carefully measured and a trial implant is inserted into the space. X-rays are taken to confirm the appropriate sizing and positioning of the trial. This must be done very precisely to ensure the mobile implant will function as desired after surgery and into the future. Once this has been determined, the permanent implant is placed. The retractor is then removed, which allow the adjacent vertebrae to compress and hold the implant in position. The bone will heal into the implant itself over the coming weeks to further secure the position. Once the surgeon is satisfied that the disc is in the proper location, they remove their equipment and guide the trachea, esophagus and other tissues back to their original location before closing the incision site. A one level disc replacement procedure typically takes less than one hour to perform.
Spinal Disc Replacement Recovery
Depending on your recovery, you may be discharged home the same day as surgery.
Because surgery was performed from the front of the neck, most patients have a sore throat, raspy voice, and some achiness with swallowing for the first week after surgery. The back of the neck can be sore in the muscles. A soft collar can be used for comfort – rarely, a collar is requested to be used by the surgeon to provide additional support to the spine. Pain from the impinged nerves usually improves quickly after surgery. If weakness was present, it can take time for the nerves to reach the muscles and the muscles to strengthen. The disc is fully healed into position in about three months, at which point most patients have obtained the maximum expected range of motion.
For more information about the treatment options for neck and arm pain, reach out to Dr. Jackman and his care team today.